
South Africans of today have become accustomed to endless waiting — for almost everything. Waiting has become less of an inconvenience and more of a condition of life. Jobs, healthcare, housing, opportunity — all suspended in systems that are overstretched wholly inaccessible. Nowhere is this starker than in healthcare, where inequality determines not only quality of care, but the time it takes to receive it. And in that waiting, people are not just losing time — they are losing years of their lives.
Healthcare in SA has been overwhelmingly defined by delays — often measured not merely in days or months, but in years of discomfort, anxiety, deteriorating health and diminished dignity.
For millions of South Africans, healthcare remains a daily reminder of rampant inequality, even decades into our democracy. Public hospitals and clinics carry enormous burdens, healthcare workers operate under immense pressure, and patients are often forced to grapple with systems that treat them as wholly disposable.
Even those with medical aid frequently discover that access to treatment is not guaranteed. Procedures are delayed, declined or trapped in layers of bureaucracy. For many, quality healthcare exists in theory long before it exists in practice.
It is within this reality that the work of Dr Ephraim Kgoete demands attention.
Not because South Africa needs another feel-good story, or should romanticise the failures of our healthcare system. And certainly not because individual acts of kindness can substitute for structural reform. His story matters because it forces us to confront something uncomfortable: where our institutions have failed to care for everyone, some individuals have responded directly and decisively.
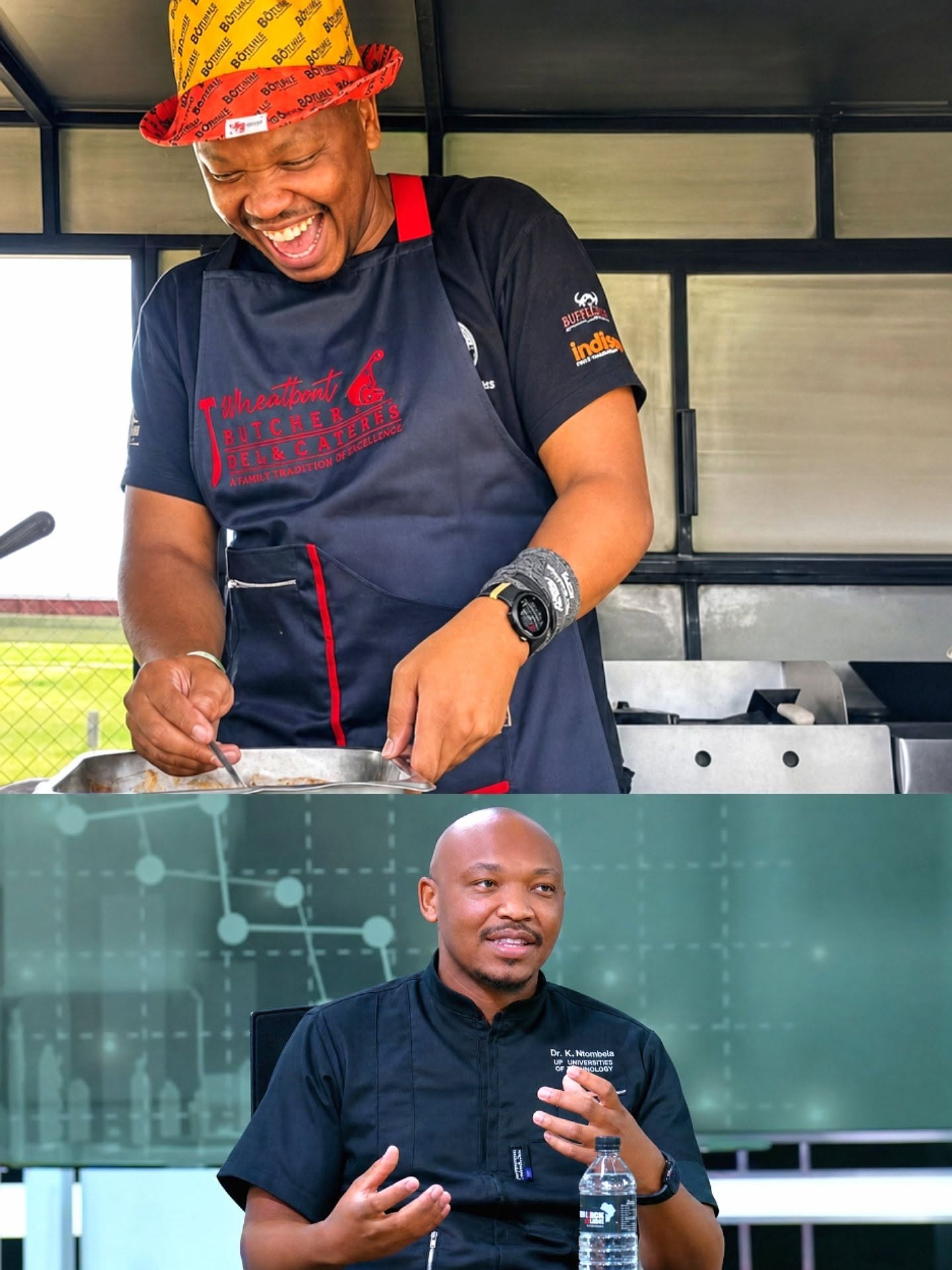
Through the Khayalami Health Foundation, Dr Kgoete (known as ‘Doctor Ya Batho‘ – or ‘The People’s Doctor’) has dedicated himself to assisting people who have fallen through the cracks of the healthcare system. As a General Practitioner from Ga-Sekhukhune, his work extends well beyond the consulting room. It involves identifying vulnerable patients, raising funds for procedures, connecting people with specialists, advocating for treatment, and mobilising support for those who would otherwise be left stranded in silence.
In many ways, his stellar work has become a bridge between communities and a healthcare system that often feels exclusionary, fragmented and inaccessible.
The significance of this work becomes clear when one looks at the lives behind it. Last year, Kgoete reportedly helped a patient who had spent a decade waiting for surgery. Ten years of waiting, of pain, uncertainty and the slow erosion of hope. More recently, he assisted Thomas Mogale, a man who lived with facial cysts for more than twenty years before finally receiving treatment. These are not simply medical cases. They are stories of prolonged invisibility in systems that are supposedly designed to reduce human suffering.

What Dr Kgoete understands is simple but often forgotten: behind every waiting list is a person. Behind every delay is a life suspended. Behind every statistic is someone learning, over time, to expect less from the system meant to care for them.
That refusal to normalise invisibility is the foundation of his work.
It is also why his story calls to mind the late Dr Gomolemo Mokae, popularly known as “The People’s Doctor”. Dr Mokae, who opened his surgery in a shack in Ramagodi near Brits, was famous for treating destitute patients free of charge, and making-up for the deficits through the paying patients who were on medical aid. These two contexts differ, but they belong to the same tradition: a view of medicine that cannot be separated from dignity, justice and social reality.
Dr Mokae, a stalwart of the Black Consciousness Movement (BCM) and the Azanian People’s Organization (AZAPO), understood that health is never just biological. It is political and social. A sick society produces sick bodies. A society structured by exclusion reproduces suffering in clinical form. Dr Mokae was brutally murdered whilst sleeping in his Ga-Rankuwa home north of Pretoria on March 5, 2025. His killers are yet to be brought to book.

That same understanding of Dr Mokae runs through Dr Kgoete’s work. He is not merely treating conditions. He is intervening in the consequences of inequality. He is stepping into the space where poverty, exclusion and institutional limits leave people waiting too long for care that should have come earlier. In doing so, he reframes healthcare as something more than service delivery. It becomes an act of recognition. A declaration that people who have been forgotten still matter.
What makes this more striking is how he chooses to operate. At a time when many young South Africans feel disillusioned by the gap between education and opportunity, his example disrupts easy narratives of success. We are told that qualifications guarantee stability, yet many graduates find themselves unemployed, underemployed or working far from the industries they had planned for. The frustration is real and widely shared.
Yet, here is a medical doctor who is also known for selling kotas, all while using his resources to help fund life-changing medical procedures for vulnerable patients. In a society obsessed with status, that carries immense weight. It challenges the idea that dignity is tied to prestige. It shows that purpose can exist outside formal recognition. There is nothing degrading about honest work when it is done in service of others. If anything, it becomes more dignified when it is rooted in responsibility rather than image.
This is also why Dr Kgoete’s story sits comfortably within a broader African belief-systems of Ubuntu and Pan-Africanism.
Too often, Pan-Africanism is reduced to speeches and symbolism, stripped of its practical meaning. Yet at its core lies a simple proposition: our lives are inter-connected and inter-dependent. The wellbeing of one person is tied to the wellbeing of others. Suffering is not meant to be isolated. Responsibility is not meant to be individualised. What Dr Kgoete is doing is a lived expression of that principle. He is demonstrating that healthcare is not only a transaction between doctor and patient, but a communal obligation. It is a reminder that no society can claim progress while large portions of its people remain locked out of basic care.
Above all, South Africa still desperately needs healthcare reform. It still needs better funding, stronger institutions, shorter waiting lists and greater access to quality treatment. None of that disappears because of a single doctor’s extraordinary work. There is still much more to be done.

But while systemic change remains urgent, so too is recognition of those already acting within the cracks of the system. Because people like Dr Kgoete remind us of something easy to forget in times of strain: that progress is not only built through policy, but through presence. Through those who choose not to ignore suffering, but address it. Through professionals who understand that success loses meaning when it is disconnected from service to the people. Through communities that continue to care even when systems consistently fail to do so.
As Dorothy Day once beautifully said: “People say, ‘What is the sense of our small effort?’ They cannot see that we must lay one brick at a time, take one step at a time. A pebble cast into a pond causes ripples that spread in all directions. Each one of our thoughts, words and deeds is like that.”
We all know that there is much to criticise about South Africa’s healthcare system, and much of that criticism is extremely justified. But if we are serious about building a better tomorrow, we must also learn to recognise and protect those who embody the values we claim to believe in today. Those who choose to act, and make a palpable difference. Not because they’re solving everything, but because they remind us that a beautiful, equal, empowered South Africa is still possible. And at times like these, that reminder is the most potent medicine we have.















![SOUTH AFRICA SECURES OVERWHELMING SUPPORT AT ILO COMMITTEE ON APPLICATION OF STANDARDS - image: Department of Employment and Labour via Facebook]](https://gsmn.co.za/wp-content/uploads/2026/06/714264670_1472392264930586_8685705720856437543_n.jpg)

